
I remember vividly the conversation my husband and I had with my oncologist the day he shared my diagnosis and treatment protocol. He told us the protocol for high risk Acute Promyelocytic Leukemia would consist of two and a half years of treatment broken into four cycles. Each of the first three cycles would consist of 30-36 days and the last cycle, 24 months. Hearing that was almost as devastating as hearing, ‘You have leukemia’. As the mom of young daughters, the idea of being unwell, unavailable, unable to provide for my family during such a critical time in their lives made me feel utter despair. Like an utter failure.
Just when I thought it couldn’t get any worse, he finished with, ‘the prognosis for survival is 90%…as long as you make it through the next 10 days‘. What I had just learned was inconceivable no matter how hard I tried to process it. The only thing I could do to prevent myself from going off the deep end was take things one step at a time. One minute at a time if need be. Based on the, ‘as long as you make it though the next 10 days’, statement, it was very clear what my first goal would be; live through the next 10 days.
They may have been the easiest of any 10 days in treatment. The fact is, my body was failing at the point of admission but there wasn’t much pain. I knew my life was in danger; how close I was to the end but the primal need to survive was so strong I just didn’t feel much. Every single waking moment, action, thought was reserved for one purpose and one purpose alone – stay alive. In a way, it was a blessing.
I was fortunate to have a big support community that helped with my home and my children. I told myself regularly that I only had 60 days left, 45 days left, 30 days left, until I would not longer need to be at the hospital, 65 kilometres away from home, daily. Until then, I knew my family was in good hands. One of my daughters teachers would even regularly text me pictures of her from the classroom just to ease my mind.
The end of my IV treatment came in April 2018. I sat in a chair in Outpatient Day Services for the last time receiving Arsenic Trioxide. I must say, it was an incredibly anti-climactic day. My Mom drove me in that day – I still wasn’t strong enough to drive safely – so she and I sat there at the hospital while I received my 87th infusion of Arsenic Trioxide. When the bag emptied and that relentless ‘Infusion Complete’ beeping started, I was as excited as a person infused 87 times with arsenic could be. I was done and, God willing, I wouldn’t have to sit in one of these chairs ever again.
This phase of treatment was closed out, not by the ringing of the bell, but with my fourth bone marrow biopsy. I always find it fascinating that the majority of people don’t find bone marrow biopsies painful. Uncomfortable, for sure, but most don’t think they are painful. All of the three biopsies before it, I found to be painful. Truth be told, I’m not sure if it’s that they are so painful for me or the complete feeling of helplessness when my bone is being broken with what essentially looks like a straightened cork screw. Just the knowledge that such a thing has to happen or I could die, that I really don’t have an option but endure such an invasion, never ceases to stir palpable anger. I digress…
I’m not really sure what I expected at this point in treatment – even whether the upcoming Maintenance therapy was considered treatment. After a four week break, following my fourth biopsy, I returned to the hospital to discuss what was next. All of the suppressed emotions I hadn’t yet dealt with from diagnosis had caught up with me by that point. However, starting maintenance felt like an accomplishment and I was optimistic! I had beat my cancer and now we were going to spend the next two years making sure it stayed gone and recovering from the ordeal. It actually felt great.
What exactly was the desired effect and outcome? According to the National Cancer Institute, the definition of maintenance therapy is ‘Treatment that is given to help keep cancer from coming back after it has disappeared following the initial therapy. It may include treatment with drugs, vaccines, or antibodies that kill cancer cells, and it may be given for a long time‘. Understanding this, the desired effect and outcome is to abolish any existing cancer cells and to keep the cancer from coming back using drugs. The effect is the white blood cells stay on the cusp of below normal range to barely normal range.
It didn’t take long for this day to become one of the most confusing days since my diagnosis. In retrospect, it was yet again, another transitional period during my treatment – similar to the experience I previously wrote about, when I had transitioning from inpatient to outpatient care (Your Role as an Inpatient, Outpatient and Transitioning Between). One of the questions I asked during that appointment was, ‘When can I go back to work?’. My oncologist responded with, ‘Now’. For a moment, I actually felt like it was a stupid question to ask in the first place. I mean, my time would no longer be consumed with daily appointments so maybe the expectation was I go back? My next question was, ‘Can I garden now?’. His reply solidified that, indeed, I was asking stupid questions. He said, ‘Why couldn’t you?’ *Insert shoulder shrug here*
Next, I found it interesting that my oncology team didn’t really consider maintenance to be chemotherapy. In fact, a few of the interesting things I began to realize are, different people within the hospital had different thoughts and expectations of maintenance. Some consider it chemotherapy, some don’t. Some consider the medications cytotoxic, some don’t. Some believe that life returns to ‘normal’ after IV treatment finishes. I’m here to tell you, it does not.
Let’s explore this a little more. According the the National Cancer Institute, chemotherapy is defined as, ‘Treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing’. It would seem that this definition is consistent with maintenance therapy. It may seem trivial to spend much time thinking of such a minor detail as to whether medical professionals believe maintenance to be chemotherapy but let’s look at this from the perspective of a recovering cancer patient.
Imagine for a moment waking up to your incessant alarm clock one morning and feeling worse than you ever have. You don’t want to go to work so you hit the snooze button 2 or 3 times. Maybe you convince yourself to get up and go. Maybe you don’t. Maybe you feel so horrible that you can’t think straight, or maybe your body hurts so bad from the flu so you just turn off your alarm, take some Benadryl and go back to bed hoping to sleep it off. To a cancer patient, this sounds like heaven. Why? Because unless you’re willing to gamble with your life, it isn’t an option. It doesn’t matter how terrible you feel, how capable you feel or are. You have to get out of bed, you have to go to the hospital or take those pills that will, inevitably, make you feel even worse than you already did.
If the torture of self-management isn’t enough, such an illness invites a ton of other organizations into your personal life including medical organizations such as your hospital of care, primary care physicians, support clinics, local government run health organizations such as the Local Health Integrated Network in Ontario, insurance companies, your own employers and the Canada Revenue Agency.
If a recipient of the cancer lottery is so lucky to have insurance coverage, they are not only responsible for being present throughout their own treatment, they are also accountable to some of the aforementioned organizations. Even in the event that a patient has a compassionate and understanding employer and insurance company, the situation itself creates a significant amount of anxiety. While anxiety, as we know, is caused by our lack of control of any given situation, makes fear of the unknowns that much worse. For example:
- Will you be eligible for your full wages?
- How much money will you lose while on disability?
- Will you still be able to pay your bills, save for your childrens education or save for your own retirement?
- Do you have life insurance in case things go bad?
- Will you have full benefits and if so, for how long?
- Will you go back to your own job?
- Will you lose your job?
- When will you be physically able to go back to work?
- Do you commute?
- How sick is too sick to work?
- Will they believe you?
- Will you get approved for CPP Disability if you’re expected to be away from work for an extended period?
- When will they call for the next update?
- If you don’t answer their call, will they think you’re avoiding them?
In the past, some of these questions were far less commonly asked. As cancer used to be mostly reserved for the older generations, re-entering the workforce or saving for retirement may not have been a topic of discussion. As young adults, these uncertainties combined with lack of clarity that inconsistencies in messaging or no messaging at all can create, make a difficult situation that much more stressful. Ultimately, depending on the answers, may even have a severe impact on the remainder of a survivors quality of life.
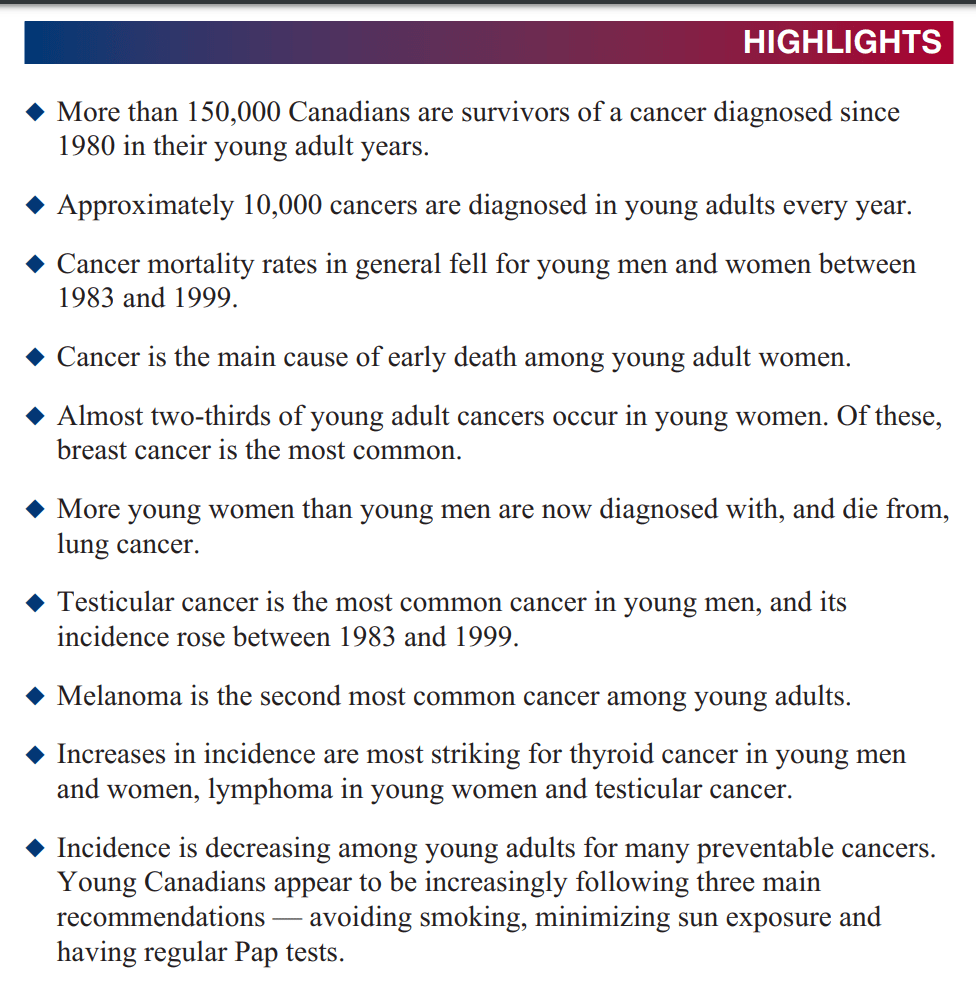
As we know, survivors are living longer after cancer. What we don’t hear about as often is that cancer is impacting people much earlier in life. Here are some examples. Click the images to see the full articles.

Even as far back as 2006, studies can be found on the impact of cancer on young Canadians…
In the United States, there is even a shorter life expectancy for those under 65 years old than there has been in recent decades (Reframing Healthcare, Zeev E. Neuwirth)!
Whether it be cancer, gastrointestinal disease, obesity, diabetes, stress disorders, we are getting sicker. This is clearly evidenced in the fact that young people are expected to die sooner than our predecessors. There is a plethora of studies that evidence the same due to various environmental factors, as I’ve noted in one of my previous articles, Environmental Dangers: Social and Political Influences and Diet. However, today I want to focus on what the lack of consistency, clarity, communication and resources all means to the young adult patient in a medical setting.
We are children, students, young moms and dads, new husbands and wives. We are in the stages of life that require ambition, focus and growth, that demand responsibility and accountability. We can not push aside these things because, thanks to advances in cancer treatment, there will, more so than previously, likely be life after cancer. We will deal with social isolation, stunted career growth and financial security, infertility before some of us have even thought about children, we will be separated from our children while we endure treatment. As students, we may have to, and moreover, NEED to finish school more than ever before. We may be driven to achieve things we never thought we could because we stared death in the face and gave it the middle finger. Our fire may burn brighter than ever before, helping us to lead our children on the path of humanity, humility, gratitude because we now know what it’s like to be isolated, mislead, outright lied to and we hope to build a more compassionate future. It means that we will not tolerate being treated like a disease. It means that we are in dire need of rehabilitation resources so we can get back to our family, life, emotional wellbeing. It means that we expect our medical team to be understanding of our unique challenges. It means we expect transparency and vigilance because we have enough to deal with without having to research every piece of information we’re given for accuracy. That’s assuming someone is assertive and savvy enough to do so. For those who are not, in some cases, the results can be devastating, even deadly.
When I was a young girl, my mom used to tell me, ‘never kick people when they are down. Instead, help them up’. This defines humanity and as my experience both prior to and since my cancer diagnosis, this is something that is clearly lacking in the healthcare space, not necessarily through the fault of the people, or maybe so but definitely as a result of the government and college oversights. This was so bewildering to me that I felt the need to reach out to various medical institutions to understand the healthcare providers experience. I participated in three training sessions offered by the Local Health Integrated Network. These training sessions are typically only provided to medical professionals province wide but I was invited to participate. What I learned was eye opening. There are already medical institutions which are trying to reframe the healthcare experience! Each and every one of those training sessions had the same resounding message, though entirely different topics; in order to achieve maximum adhereance, best outcomes, and outstanding patient experience, PATIENTS MUST BE TREATED WITH DIGNITY, RESPECT, COMPASSION AND UNDERSTANDING. When our medical professionals don’t appropriately assess, communicate, share information, validate our concerns, or worse yet – lie to us for liability purposes, they have lost our trust. When their governing bodies restrict them from being open and honest, we have an even bigger problem. And don’t kid yourself, it IS happening.
When I began maintenance therapy, I was told that I could begin resuming my life; finding my new normal. I was told my medications shouldn’t impact my quality of life and while I may want to be mindful of how quickly I hit the ground running, I was led to believe the remainder of treatment would be smooth sailing. In fact, I was even told one of the medications may resolve the extreme joint inflammation which plagued me since starting chemotherapy.
The fact is, the last eighteen months of maintenance therapy were the darkest days of my life. Recovering from cancer treatment is no small feat. The introduction of maintenance medications has most certainly compounded some of the effects of chemotherapy. While I was told to expect to resume normal life, my body continued to get rocked by extreme joint inflammation which progressed throughout my entire body. Some days so bad I wished I never woke up. Some days, the fatigue scaring me so badly that I would text my husband to let him know where I was in case I didn’t make it home because I couldn’t function well enough to drive. I even recall reporting the onset of mood swings and depression at the beginning of each cycle to my medical team. How quickly my mind would clear during the off time was outstanding. Then, the next round of methotrexate would begin and it felt like I hit a gray haze of sadness and increasing anger. My association with the start of that particular drug and my mood changes quickly dashed and the recommendation to make an appointment with a mental health professional was infuriating. Ultimately it also resulted in my decision to stop most of my maintenance drugs one year early.
Let me be very clear. I understand that it is unreasonable to expect everyones experience to be the same and therefore, forecasting the effects of treatment is not accurately possible. But for the same reason, invalidation of patient concerns should never happen. I am also quite understanding of the fact that medical training, although changing, isn’t heavily focused on dealing with patients emotions. In other industries, particularly those which are already more consumer centric, the concept of emotional intelligence has only recently been recognized. The only assumption that can be made is, medical teams are simply not widely trained to handle the changing landscape – younger patients with unique challenges and higher expectations. I understand, at least in small part, the pressure put on them by the government to adhere to insanely stringent administrative requirements. I am even able to empathize with the governmental pressure now that I’ve been through my first income tax season as a sick person (look out for an upcoming article on how to handle income tax and medical expenses)!
What is boils down to is, we need the same in return. Understanding, empathy, compassion, the respect of being treated like human beings. We are NOT our disease. We are NOT a patient number. We are NOT an insurance claim number. We are human and we deserve our dignity. This is a call to action.
No matter what the medical condition, the one thing we need above all else is to be treated like human beings. The cancer community and the chronic illness communities are calling on the Canadian medical industry to do what needs to be done to inject humanity into medical care and start reframing healthcare to put the patient first.
In the absence of trust, compassion, empathy and humanity, Canadians will continue to suffer and even die needlessly.
We need your help.
Until next time, we’ve got this!

The phrase that my health team always used to answer many of my questions was ‘everyone is different’ It drove me crazy because it was hard to plan physically and emotionally for the unexpected.
I also feel that my delayed diagnosis was due to the fact that Doctors were not taking me serious. In chatting with other cancer patients across Canada I have discovered that we all have different health care systems but they all have room for improvement.
LikeLike
Hi CJ,
There have certainly been desperate angry moments where I’ve blamed my medical team for the unexpected.
Like you, I called my doctors office twice leading up to diagnosis and wasn’t taken seriously…then had to insist being allowed to see a doctor at my local hospital. I can’t really even explain that one. By the time I was diagnosed my blood composition was 90%. They were shocked I walked in on my own two feet!
It has been an incredible learning experience! You’re right, many systems, many good people and some room for improvement!
LikeLike